Breakthroughs in Bipolar Treatment
"We should continue to repurpose treatments and to recognise the role of serendipity" (Geddes & Miklowitz, 2013).
That quote was from a recent review article in The Lancet, which did not hint at any impending pharmacological breakthroughs in the treatment of bipolar disorder. In other words, the future of bipolar treatment doesn't look much different from the present (at least in the immediate term).
Bipolar disorder, an illness defined by the existence of manic or hypomanic highs, alternating with depressive lows, can be especially difficult to treat. And the mood episode known as a mixed state, where irritability, expansive mood, anxiety, and/or agitation occur simultaneously with depressive symptoms, is an under-recognized, moving-target diagnosis (Koukopoulos et al., 2013). Mood stabilizers such as lithium and divalproex have long been the first line pharmacological choices. But these don't always work, and polypharmacy seems to be the rule, rather than the exception.

The spinning molecule above is haloperidol, a first generation antipsychotic drug developed in 1958 and approved by the FDA in 1967 as a treatment for schizophrenia. It's a dopamine blocker known for producing untoward extrapyramidal side effects, or movement disorders such as tremors and tardive dyskinesia. Nonetheless, haloperidol (Haldol®) is still the most effective drug for the acute treatment of mania, and fairly well tolerated (see HAL in the figure below). The second generation (atypical) antipsychotics risperidone (RIS) and olanzapine (OLZ) also turn out pretty well in the antimanic sweepstakes. But these drugs can also have untoward side effects, notably substantial weight gain that can lead to high cholesterol, diabetes, and metabolic syndrome.

Figure (Geddes & Miklowitz, 2013). Ranking of antimanic drugs according to primary outcomes derived from multiple treatment meta-analysis. Efficacy is shown as a continuous outcome against the dropout rate. Treatments toward the red section combine the worst efficacy and tolerability profiles and treatments towards the green[ish] section combine the best profiles.1
Clearly, effective medications with fewer side effects are needed. Unfortunately, there doesn't seem to be anything new on the horizon, according to Geddes and Miklowitz:
Overall, advances in drug treatment remain quite modest. Antipsychotic drugs are effective in the acute treatment of mania; their efficacy in the treatment of depression is variable with the clearest evidence for quetiapine. Despite their widespread use, considerable uncertainty and controversy remains about the use of antidepressant drugs in the management of depressive episodes. Lithium has the strongest evidence for long-term relapse prevention; the evidence for anticonvulsants such as divalproex and lamotrigine is less robust and there is much uncertainty about the longer term benefits of antipsychotics.
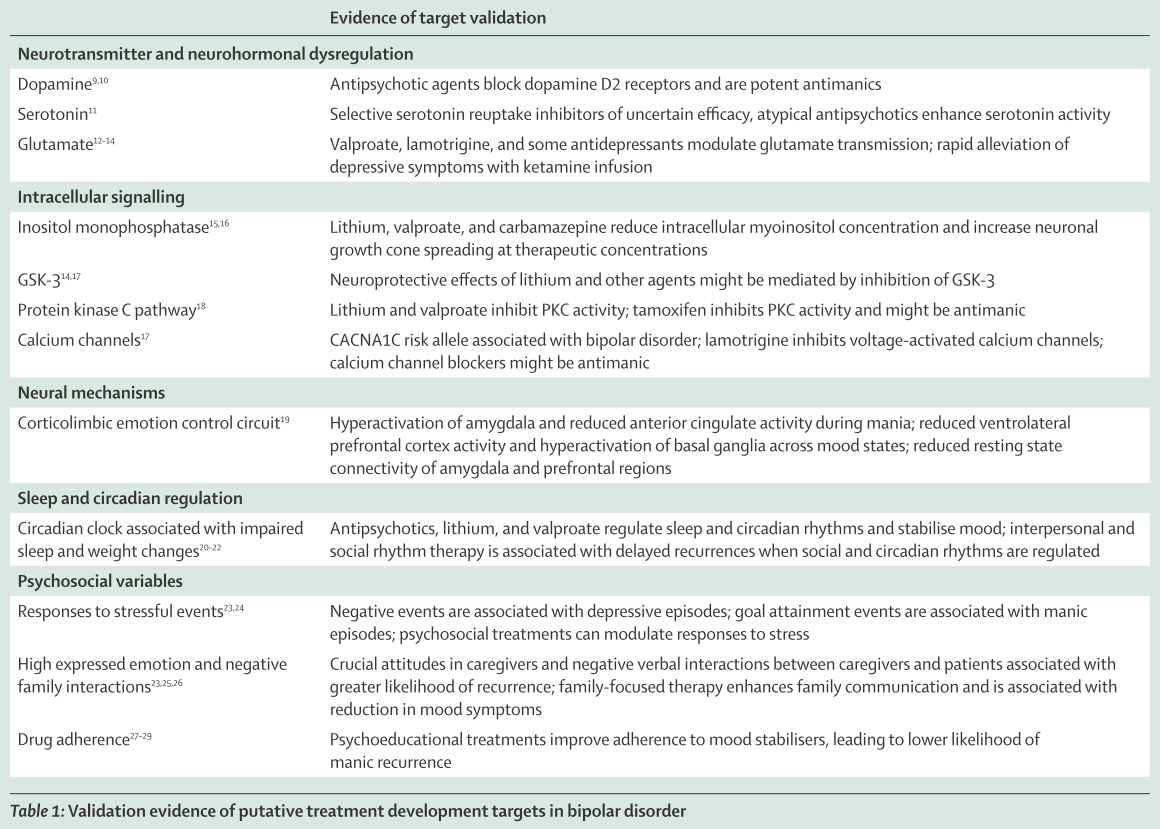
The article is actually more bullish on combining existing drugs with various psychosocial interventions (e.g., family-focused approaches, strict regulation of social and circadian schedules, etc.), which are touched on below in the Appendix (Table 1 of Geddes & Miklowitz, 2013). That table also mentions some of the usual drug suspects.
To find out what else might be in the works, I looked through ClinicalTrials.gov for open interventional drug studies in adults. There were a few surprises... foremost among these was Methylphenidate for the Treatment of Acute Mania. It seems bizarre to me that methylphenidate (the stimulant drug Ritalin) would be proposed as a treatment for mania, since 40% of patients prescribed stimulants for bipolar depression (or comorbid ADHD) experienced stimulant-induced mania/hypomania (Wingo & Ghaemi, 2008).
The Ritalin trial was submitted to ClinicalTrials.gov in Feb. 2012, but the study is not yet open for patient recruitment 1.5 years later. The investigators recently published the study protocol in BMC Psychiatry, however (Kluge et al., 2013). They proposed the ‘vigilance regulation model of mania’ where:
Unstable vigilance induces a pathogenic circle with vigilance stabilisation syndrome leading to full-blown mania. [NOTE: huh?]
The outlined model ... is related to personality theories about extraversion [9] and sensation seeking [10] which comparably explain these traits as an attempt to compensate for low central nervous system arousal.
Basically, it works for ADHD, and there are a handful of uncontrolled case reports, so.... let's conduct a clinical trial.
Bipolar Depression
Depressive episodes in bipolar disorder are longer in duration and considered more difficult to treat. Again, ClinicalTrials.gov did not disappoint, revealing a grab bag of "repurposed" treatments:
Adjunctive Lisdexamfetamine - another stimulant for ADHD (aka Vyvanse).
Adjunctive Isradipine (a calcium channel blocker prescribed for high blood pressure) - this idea — not a new one — deserves a post of its own.
Adjunctive Minocycline (an antibiotic) - the proposed mechanism of action is to reduce the production of pro-inflammatory cytokines.
Ceftriaxone (another antibiotic) - however, the proposed mechanism here is inactivation of the excitatory neurotransmitter glutamate, via actions on the glutamate transporter.
NMDA Antagonists (i.e., club drug ketamine) - this is complicated and again deserving of its own post.
Tranylcypromine (a monoamine oxidase inhibitor) - old, old school antidepressant with lots of contraindications and dietary restrictions.
Ramelteon (a melatonin receptor agonist used to treat insomnia) - targeting the sleep/wake cycle could be an important approach.
N-Acetyl Cysteine and Aspirin - aspirin? really??
We propose to conduct a double-blind placebo-controlled trial with a widely available and prototypical non-steroidal anti-inflammatory agent, aspirin, and an antioxidant agent, NAC, involving symptomatic Bipolar Disorder type I and II patients having a depressive or mixed episode currently. This will be the first controlled study to test the hypothesis that aspirin and NAC, by themselves or in combination, will be beneficial in treating depression in bipolar disorder patients and in promoting mood stabilization.

For the ultimate in repurposed treatments, see this recent opinion piece in BMC Medicine on Aspirin: a review of its neurobiological properties and therapeutic potential for mental illness.
Footnote
1 Abbreviations for Geddes and Miklowitz (2013) Figure: ARI=aripiprazole. ASE=asenapine. CBZ=carbamazepine. VAL=valproate. GBT=gabapentin. HAL=haloperidol. LAM=lamotrigine. LIT=lithium. OLZ=olanzapine. PBO=placebo. QTP=quetiapine. RIS=risperidone. TOP=topiramate. ZIP=ziprasidone.
References
Berk M, Dean O, Drexhage H, McNeil JJ, Moylan S, Oneil A, Davey CG, Sanna L, & Maes M (2013). Aspirin: a review of its neurobiological properties and therapeutic potential for mental illness. BMC medicine, 11 (1). PMID: 23506529
Geddes JR & Miklowitz DJ (2013). Treatment of bipolar disorder. Lancet, 381 (9878), 1672-82. PMID: 23663953
Kluge M, Hegerl U, Sander C, Dietzel J, Mergl R, Bitter I, Demyttenaere K, Gusmão R, Gonzalez-Pinto A, Perez-Sola V, Vieta E, Juckel G, Zimmermann US, Bauer M, Sienaert P, Quintão S, Edel MA, Bolyos C, Ayuso-Mateos JL, & López-García P (2013). Methylphenidate in mania project (MEMAP): study protocol of an international randomised double-blind placebo-controlled study on the initial treatment of acute mania with methylphenidate. BMC psychiatry, 13. PMID: 23446109
Koukopoulos A, Sani G, Ghaemi SN. (2013). Mixed features of depression: why DSM-5 is wrong (and so was DSM-IV). Br J Psychiatry 203:3-5.
Wingo AP, Ghaemi SN. (2008). Frequency of stimulant treatment and of stimulant-associated mania/hypomania in bipolar disorder patients. Psychopharmacol Bull. 41:37-47.
Appendix
- click on image for a larger view -
posted by The Neurocritic @ 2:22 AM
20 comments
![]()
![]()
Subscribe to Post Comments [Atom]













20 Comments:
Part of the effective treatment of bipolar is good social supports, and it helps a lot to have a partner with an interest in being part of the approach.
Thanks for this great update.
How could Zyprexa be ranked first for acceptability? I mean you take that drug and you get fatter than Aunt Marge Dursley of Harry Potter fame! The bar for "acceptability" must have been set pretty low in this study!!!!!
Anonymous - Good point. I should have clarified that the "acceptability" rating was for short-term use to stabilize the manic episode (acutely), rather than long-term use for maintenance therapy (chronically). In their quote, the authors express uncertainty about the benefits of long-term use.
Sandra - You're quite welcome.
The idea of testing Ritalin may not be as crazy as it sounds. There is an old literature on use of amphetamine in mania. Below is the Medline entry for a German report from the 1970s. But I would see it more as a tool for studying underlying processes in mania than as a potential treatment.
D-Amphetamine in manic syndrome (author's transl). [German]
Beckmann H. Heinemann H.
Arzneimittel-Forschung. 26(6):1185-6, 1976.
[Clinical Trial. English Abstract. Journal Article]
UI: 786316
Abstract: Six manic patients were acutely treated with 30 or 50 mg d-amphetamine, respectively. There was no intensification in any of these patients of gross manic behavior or single manic symptoms. Conversely, there was sedation and considerable reduction of manic symptomatology in all of them. This effect lasted for 1 to 3 h only. The clinical subgroup "elated-grandiose" was significantly, the subgroup "paranoid-destructive" was not significantly influenced. "Drive" and "mood" were similarly reduced. There was, however, no complete recovery from mania.
It's a shame we don't get to see where cannabidiol sits on that chart, I presume to the north east?
So cannabinoids for the affective disorder, cannabinoids for psychosis, cannabinoids for metabolic syndrome, cannabinoids for diabetes and cannabinoids for autism.
Whatever next?
Hey, I comment sometimes on your blog. If you would, allow me a moment for some quick beseeching.
Five years ago I earned a BA in psychology. By the time I'd finished the degree, I was determined to make it as a fiction writer, but the pursuit has petered out. I think my scope was too vaguely broad, while my editing, too compulsive. It allowed me to misread my endless shifting of words as "incremental progress," and fractured whatever narrative I'd begun with into dry exercises of technique. Incidentally, I think that's what would make me good at science. I've been studying for the GRE and I needed recommendation letters. I know your anonymity makes this a long shot, but I thought I'd throw it out there. I wouldn't expect a letter on the merit of a few diverting comments, of course. I could do remote editorial or secretarial work, or whatever's needed. I've got a pretty flexible skill set.
Thanks for your time!
I just read the paper in Lancet by Geddes and Miklowitz. It is a workmanlike summary of recent efforts to improve the treatment of bipolar disorder, with a welcome emphasis on psychosocial treatments. What stands out, however, is the authors’ stunning empiricism. They discuss no underlying constructs except reflexively from drug considerations. In this defenseless empiricism they are, of course, at one with DSM-5.
Where is a discussion of pathophysiology? Where is a discussion of conceptual models of bipolar disorder, like the Carroll-Klein model? Or of hemispheric lateralization – called to our attention by Flor-Henry decades ago for mania? Where is a discussion of secondary manias resulting from brain lesions and what do these teach us?
Where is a discussion of the cholinergic system – Janowsky’s seminal work on acute physostigmine effects in mania? Or of the noradrenergic system – MHPG differences between depression and mania? Or of the nosologic relationship between mania and depression? Are these opposite poles of one disorder or are they separate disorders that sometimes co-occur? Was Emil Kraepelin right after all with his spectrum concept and did Karl Leonhard lead us all astray by coining the term bipolar disorder? Where is a discussion of mixed states? Why do we use anticonvulsant drugs? What evidence makes that approach seem viable? Did Robert Post lead us astray with speculative talk about kindling in bipolar disorder? That was the prelude to use of anticonvulsants.
What does the term anti-manic mean when applied to a drug like haloperidol or its successors? A favorite clinical pearl from the 1970s at St. Elizabeth’s Hospital in Washington, D.C., concerned a patient arrested by the Secret Service for climbing the White House fence with a personal message for the President. He was transferred to St. E’s where a diagnosis of mania was rendered. After a week on haloperidol, his boisterous overactivity and pressure of speech had subsided. In a ward conference the nurses agreed that he could now be allowed telephone privileges, whereupon he walked calmly to the telephone and dialed the White House! The point of this pearl is that drugs may have only partial effects on a syndrome like mania. The dopamine blocker haloperidol helps to control the impulsivity and overactivity of a manic patient but then it just provides a dopamine brake until the manic thought disorder resolves in due course. But when measured with an operational instrument like the Young Mania Scale, haloperidol can appear to be ‘anti-manic.’ It would have been nice to see Geddes and Miklowitz address some of these nuances.
Full disclosure: I trained in Melbourne where John Cade, the person who introduced lithium for mania, was one of my teachers. Since the late 1980s, lithium has been systematically trashed for potential toxicity by KOLs promoting newer drugs. It does not deserve to be placed where it is on the Figure by Geddes and Miklowitz, especially for long term use.
J. F. Aldridge - Unfortunately, I don't think a letter from an anonymous entity will help you that much... good luck, though.
Dr. Carroll - Thanks for your nice summary of overlooked ideas in the history of bipolar disorder(s). I think the plural is key, because the more we learn about the tiny increment of risk each identified SNP can account for, the more we can suspect that every person has a different disorder.
Neurocritic: can we maybe meet in the middle? It seems to me unlikely that “every person has a different disorder.” I lean to an analogy of mood disorders with Parkinsonism, where there is an original landmark description now known to have several different gene bases, plus a bunch of look-alike conditions that show Parkinsonian features but whose pathologies are quite different from so-called idiopathic Parkinson’s disease.
Currently I am pushing the term Kraepelin’s disease for what he called manic-depressive illness in his landmark description. Within KD there may be distinct genetic variants, as in PD. Then, surrounding KD there are probably look-alike disorders. One would be what is now called vascular depression, analogous to vascular Parkinsonism.
Dr. Carroll - Yes, that was a little hyperbolic... and based on hypothetical genetic/epigenetic factors, rather than symptoms. But the medication combination that works from person to person is so highly variable.
What do you think of Koukopoulos and Ghaemi's 2009 paper, The Primacy of Mania?
OK, I just re-read The Primacy of Mania, which appeared in 2009. I respect and enjoy the company of both authors, Koukopoulos and Ghaemi, but I have reservations about their thesis. Their synthetic review posits that mania is the primary mood disorder, that “mania is the fire and depression is its ash.” It is pretty speculative and it contains a good deal of special pleading. The most important concern for me is their equating agitated depression with a form of manic excitement. I don’t agree. Donald Klein pointed out 40 years ago that the central pain component in depression leads to agitated behavior. On the other hand, the hyperactivity of mania seems rather to be driven by hedonic drive, not by avoidance of pain. So, the pressured importuning and pacing of the agitated depressed patient can’t be equated with the logorrhea and distractible, pressured behavior of the manic patient. If it is any consolation, Emil Kraepelin made the same error. But I don’t want to be seen as dissing EK because he got so much right. A more extensive presentation of these thoughts, with related references, is here: http://www.ncbi.nlm.nih.gov/pubmed/8313611
It is also worth mentioning that this article by Koukopoulos and Ghaemi has been cited only 5 times since it was published in 2009 (Thompson Reuter Web of Science). So it has not so far had a large heuristic impact.
Thanks again for your comments. It seemed like an interesting idea with treatment implications, but I agree that agitated depressives are not all bipolar. At least we didn't get BIPOLAR II½, III, III½, IV...
Bipolar disorder remains a big problem in my community in part because of a lack of good psychiatry resources. As a FP I am left to treat a significant number of these patients without as much good psych consultation as would be ideal. Thanks for the info.
I was surprised to see that Ritalin was used as a form of treatment for a manic stated person. Depression commonly results from the use of these types of drugs (ADHD meds). So the concern came to me, how could that be used to treat a condition in which the side effects are the main issue. however, I do believe that the reason these types of diseases are so common is because the there is such a gray area when it comes to the pharmacology aspect of treatment. There is not one specific drug to help all people. some need mood stabilizing meds, some antidepressants, therapy and a "drug cocktail" will help subdue the effects of being bipolar. in retrospect, there will be no sufficient cure without lots of trials. the chart above listed many medicines that I was unfamiliar with but it simply showed how many different opportunities are out there to help people struggling with this disorder. one day, hopefully there will be a guaranteed relief of mind, emotion, and physical distress that stems from manic depression and or bipolar disease.
How I Cured My Bipolar Disorder
I read that omega-3 was being used for psychiatric disorders and gave it a try for myself. It didn’t work, but I noticed that after 13 years my urine had no calcium sediments in it anymore. Before omega-3 supplements any extra calcium I ate showed up as extra urine sediment. I then read that calcium was important for proper neuron function and added calcium supplements to my diet thinking that I might not be getting enough. I increased the amount until I started seeing calcium sediments in my urine again. My mental symptoms stopped then. I believe the mechanism for the success of omega-3 is through its ability to allow the body to maintain a higher blood level of calcium. Higher calcium levels are known to reduce the level of excitability of neurons. Perhaps omega-3 allows the kidneys to reabsorb calcium to a level that satisfies all the body’s requirements.
There does seem to be some research indicating that diminished blood flow to the brain may be a contributing factor in Bipolar Disease. So NAC and aspirin could prove to be extremely effective.
In the study rating bipolar medications for efficacy and acceptability, I am curious to what extent the authors took noncompliance into consideration. The research literature shows noncompliance to be very high (e.g., http://www.biomedcentral.com/1471-244X/12/99) and my own experience in treating bipolar has been that full compliance is the exception, primarily due to the adverse side effects, concomitant disorders such as alcoholism, and the euthyrmic nature of manic episodes. Ditto for schizophrenia.
Hi,
Healthline just launched a video campaign for bipolar disorder called "You've Got This" where bipolar patients can record a short video to give hope and inspiration to those recently diagnosed with bipolar disorder.
You can visit the homepage and check out videos from the campaign here: http://www.healthline.com/health/bipolar-disorder/youve-got-this
We will be donating $10 for every submitted campaign to To Write Love On Her Arms, so the more exposure the campaign gets the more the videos we'll receive and the more Healthline can donate to research, support, and treatment programs for mental health disorders.
We would appreciate if you could help spread the word about this by sharing the You've Got This with friends and followers or include the campaign as a resource on your page: http://neurocritic.blogspot.com/2013/08/breakthroughs-in-bipolar-treatment.html
Please let me know if this is possible and if you have any questions. And, if you know anyone that would be interested in submitting a video, please encourage them to do so.
Best,
Maggie Danhakl • Assistant Marketing Manager
p: 415-281-3124 f: 415-281-3199
Healthline • The Power of Intelligent Health
660 Third Street, San Francisco, CA 94107 www.healthline.com | @Healthline | @HealthlineCorp
About Us: corp.healthline.com
Hi,
First off, I came across your site and wanted to say thanks for providing a great resource to the mental health community.
I thought you might find this bipolar disorder fact sheet helpful for your readers, as it shows symptoms, treatment and stats about the disorder: http://www.healthline.com/health/bipolar-disorder/fact-sheet
Naturally, I’d be delighted if you share this embeddable graphic on http://neurocritic.blogspot.com/2013/08/breakthroughs-in-bipolar-treatment.html , and/or share it with your followers on social. Either way, keep up the great work !
All the best,
Nicole Lascurain | Assistant Marketing Manager
p: 415-281-3100 | e: nicole.lascurain@healthline.com
Healthline
660 Third Street, San Francisco, CA 94107
www.healthline.com | @Healthline
"Very interesting blog! I really enjoyed reading it. I also write about similar topics, such as How to Deal with Regular Mood Swings & Mood Disorders. Feel free to check out my blog.
Post a Comment
<< Home