Online Gaming Addiction, Dysfunctional Families, and the Striatum

Internet addiction is perceived to be an important problem in some Asian countries, including Taiwan and Korea. Fatal marathon sessions of online gaming, in particular, have drawn a lot of media attention. Most recently, a teen in Taiwan died after playing Diablo III for 40 straight hours in an internet cafe.
Yen et al. (2010) speculated on potential cultural contributions to heavy internet use:
Internet addiction has been found to be more prevalent in some Asian countries than in the United States 1. Differences in sociocultural background might partly account for this difference. Among various Internet activities, online gaming is the most developed in many Asian countries. Commercial promotion for online gaming focuses on the adolescent population. Adolescents in high schools of Asian countries usually face a strong academic competition. Internet provides a virtual world in which they can temporarily forget the stress of academic performance.
However, "internet addiction" is a murky and controversial diagnosis that is the subject of intense debate. It is being considered for inclusion in the DSM-5, although some critics find the entire concept to be nonsensical:1
[Dr. Vaughan] Bell has argued that the Internet is not an activity, and therefore Internet addiction is a flawed idea (J Ment Health 2007;16:445–57).“Fundamentally, the Internet is a medium of communication,” says Bell, who claims that one can no more be addicted to the Internet than to radio waves. “The concept itself doesn’t make sense.”
Nonetheless, internet addiction treatment programs are blossoming in the U.S. and worldwide. Although dodgy Chinese 'boot camps' are grabbing all the headlines, another school of thought looks to family dynamics as the root of the problem.
Online Gaming Addiction: It's the Family's Fault
An unusual new fMRI paper by Han et al. (2012) examined brain activity in adolescents with heavy online game use, both before and after 3 weeks of intensive family therapy. In brief, the results seemed to suggest that activity in the dopamine-rich striatum was increased to family bonding cues after family therapy in the "addicted" gamers.2

Since I've already mentioned dopamine, you can see where this is headed. The authors cited studies on the similarities in brain activity in response to cues of affection and addiction (e.g. Fisher et al., 2005; Frascella et al., 2010), in which the striatum figures prominently. No wonder we see so many ridiculous stories on dopamine and internet addiction in the popular media.
The truth is much more nuanced. It's time to abandon the simplistic notion of dopamine as the feel-good neurotransmitter. To quote the authors of Mesolimbic Dopamine in Desire and Dread (Faure et al., 2008):
It is important to understand how mesocorticolimbic mechanisms generate positive versus negative motivations. Dopamine (DA) in the nucleus accumbens is well known as a mechanism of appetitive motivation for reward. However, aversive motivations such as pain, stress, and fear also may involve dopamine in nucleus accumbens (at least tonic dopamine signals).

The Neurocritic expanded on this thought in Is Mourning Rewarding?, and discussed the distinction between the "wanting" and "liking" aspects of reward (Berridge et al., 2009) in Great and Desperate Cures for Addiction. These two facets of reward can become uncoupled: you can continue to "want" something you no longer "like". But summaries of this research don't make good cover stories for Newsweek.
Dysfunctional Family Circus
Back to Han et al. (2012):
An association between dysfunctional family structure and adolescent substance use has been suggested by several public health studies... . . . In a study of family factors contributing to internet addiction, Yen et al. (2007) reported that higher levels of parent-adolescent conflict and lower family function were associated with internet addiction. China's “left behind children,” due to parental migration from rural to urban areas for work, have been reported to be at increased risk of physical inactivity, internet addiction, and smoking (Gao et al., 2010). In a study of 1369 university students, Tsai et al. (2009) reported that deficient social support was a significant risk factor for internet addiction...
The participants in their study were 15 adolescents with potentially problematic online gaming habits (mean 35 hrs/week), all from dysfunctional families, and 15 adolescents with no gaming issues (mean 3 hrs/week) from intact families. The criteria for problematic online game play were:
1) game playing time greater than four hours per day and 30 hours per week; 2) Young Internet Addiction Scale (YIAS) scores greater than 50. In an epidemiology study of Korean school students, Yoo et al. (2004) reported that 14% of students met the criteria of problematic internet addiction using a standard of IAD > 50; and 3) impaired behaviors or distress due to excessive on-line game play which are modified from DSM-IV criteria for substance abuse.
There were no gaming addicts from happy families in this study. Exclusionary criteria included a history of psychiatric illness, substance abuse, or neurological disorders. This is fairly important, as the literature typically notes a high comorbidity of other psychiatric disorders (e.g. depression, anxiety) along with excessive internet use.

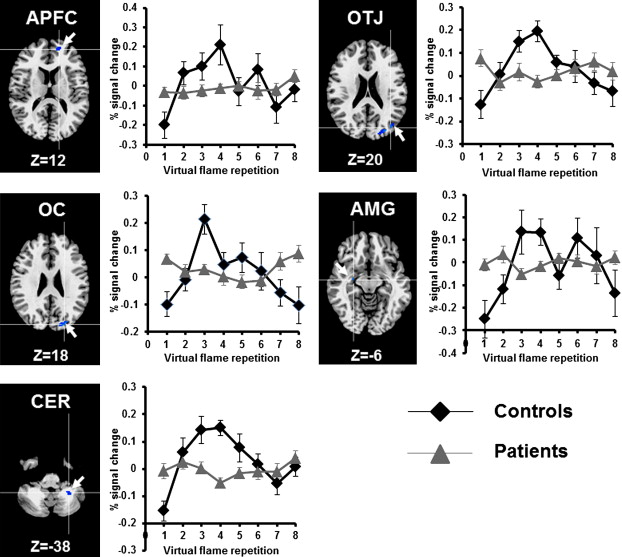
The fMRI study involved passive presentation of pictures in a block design. The stimulus categories were neutral (e.g. tree, book, chair), affectionate families (e.g. parents hugging their child, a mother kissing her child, a family birthday party), and game scenes from the preferred game, which included Lineage®, Sudden Attack®, World of WarCraft®, AION®, Dungeon and Fighter®, and StarCraft®.
The results were so problematic that I'm not sure what you can conclude from this study. Absolutely no regions in the entire brain were significantly activated (p<.05 corrected) by the happy family pictures. This was true in the gamers (both before and after therapy) AND in the control kids. For starters, if you're not going to find significant activation of the fusiform face area in a contrast of faces vs. trees you're in trouble. Also, if you're trying to make the case that affection is (or should be) rewarding, you'd better report activation of reward-related areas.
Furthermore, the game-related stimuli elicited NO significant activation anywhere in the addicted subjects' brains prior to therapy. After treatment, the gaming pictures showed greater activation than the neutral pictures in the right occipital lobe and the left middle frontal gyrus (MFG). However, the authors reported this as a reduction in left MFG from pre- to post-treatment, despite the fact that there was no significant activation in left MFG prior to therapy.
As stated earlier, the other significant treatment effect was an increase in activity in the striatum (specifically, the caudate nucleus) to the happy family photos. But again, this is problematic due to the lack of significant activity when comparing happy families to neutral. Finally, the control participants did not undergo family therapy, nor were they tested again at the 3 week time point.
Although the family therapy intervention did increase family cohesion and reduce the amount of gaming (from 35 to 12 hrs per week), I don't think we've learned anything about the neural correlates of these changes. Extensive gaming may "change your brain" [as does any other activity], but this particular study wasn't especially informative about the nature of these changes.
Footnotes
1 A leading proponent of the concept is Dr. Kimberly Young (of the Internet Addiction Center), who has developed a list of diagnostic criteria. Further, she identifies four main subtypes:
Specific net compulsions include Online Gaming and eBay Addiction. How about Etsy addiction? Regretsy addiction?
2 The results were not actually that straightforward, given the lack of statistical significance in most of the contrasts.
References
Berridge KC, Robinson TE, Aldridge JW. (2009). Dissecting components of reward: 'liking', 'wanting', and learning. Curr Opin Pharmacol. 9:65-73.
Faure A, Reynolds SM, Richard JM, Berridge KC. (2008). Mesolimbic dopamine in desire and dread: enabling motivation to be generated by localized glutamate disruptions in nucleus accumbens. J Neurosci. 28:7184-92.
Fisher H, Aron A, Brown LL. (2005). Romantic love: an fMRI study of a neural mechanism for mate choice. J Comp Neurol. 493:58-62.
Frascella J, Potenza MN, Brown LL, Childress AR. (2010). Shared brain vulnerabilities open the way for nonsubstance addictions: carving addiction at a new joint? Ann N Y Acad Sci. 1187:294-315.
Han DH, Kim SM, Lee YS, & Renshaw PF (2012). The effect of family therapy on the changes in the severity of on-line game play and brain activity in adolescents with on-line game addiction. Psychiatry research, 202 (2), 126-31 PMID: 22698763
Yen CF, Yen JY, Ko CH. (2010). Internet addiction: ongoing research in Asia. World Psychiatry 9:97.
APM = Actions per minute
Ask a Korean! explains Why is StarCraft Popular in Korea?

posted by The Neurocritic @ 1:00 AM
3 comments
![]()
![]()
Subscribe to Post Comments [Atom]